S u p e r v i s i o n o f a n A H A
 http://www.clipartbest.com/clipart-direAd47T
http://www.clipartbest.com/clipart-direAd47T
Supervision has been devised as: “the action or process of watching and directing what someone does or how something is done: the action or process of supervising someone or something” (Merriam-Webster Dictionary) to assist them effectively perform their duties.
Although most health professionals agree on the importance of ongoing supervision for quality health delivery and assist the AHAs to learn from their experience and progress in expertise, it is often overlooked or done half-heartedly. Instead of it being a participatory, problem solving,
supportive process assisting the AHA to improve their performance through feedback and reflection, those being supervised may have the feeling of being inspected with the focus on fault finding instead of providing guidance or mentoring. With no clear direction regarding roles and expectations and few or no milestones to help assess their performance,
AHAs may find it difficult to remain motivated. AHPs may lack the supervisory skills needed to effectively evaluate AHAs across the area for
which they are responsible. In addition to this, supervision may be one of many responsibilities which form part of the AHP’s scope of practice
leaving little time for adequate technical guidance and feedback to AHAs.
The Framework (The workforce, 2012) states that “while AHAs are not autonomous practitioners and always work under the overarching auspice and clinical oversight of the AHP, the degree of monitoring required will vary depending on the knowledge, experience, skill level and Grade of the AHA”. On their website, Services for Australian Remote and Rural Allied Health (SARRAH) states that an “Allied Health Assistants (AHAs) must work under the supervision of the relevant Allied Health Professional (AHPs) (i.e. tasks must be delegated to them by an Allied Health Professional). The level of supervision and monitoring will depend on the experience, skill and qualifications of the assistant and the practicalities of the work environment. Supervision may range from face to face daily interaction to less frequently and by telephone or video”. In most cases the scope of practice for assistants stating what an AHA can and can’t do is guided by the employing organisational and professional associations/regulatory bodies.
According to the Framework (The Workforce, 2012. p.25) “supervision can vary in terms of what it covers” and “depending on the context,
complexity of the task or the needs of the patients” can incorporate any of the following elements:
1. Delegation- the act of giving control, responsibility, a task or a duty to another person, in this instance the AHP delegating a task/duty to an AHA
2. Direction- assistance in pointing out the proper course of action
3. Guidance- help or advice informing an AHA what to do : the act or process of guiding the AHA through visual, verbal, manual and/or
mechanical aids
4. Support- to reassure, nurture, protect, give help or assistance to the AHA enabling them to increase their skills and confidence
5. Observation- the act of careful watching and listening; the AHP pays close attention to the AHA in order to get information
6. Joint working – or joint problem-solving involving an ongoing relationship and two-way communication between AHP and AHA (such as in Supportive Supervision)
7. Exchanging ideas
8. Coordinating activities
Although most health professionals agree on the importance of ongoing supervision for quality health delivery and assist the AHAs to learn from their experience and progress in expertise, it is often overlooked or done half-heartedly. Instead of it being a participatory, problem solving,
supportive process assisting the AHA to improve their performance through feedback and reflection, those being supervised may have the feeling of being inspected with the focus on fault finding instead of providing guidance or mentoring. With no clear direction regarding roles and expectations and few or no milestones to help assess their performance,
AHAs may find it difficult to remain motivated. AHPs may lack the supervisory skills needed to effectively evaluate AHAs across the area for
which they are responsible. In addition to this, supervision may be one of many responsibilities which form part of the AHP’s scope of practice
leaving little time for adequate technical guidance and feedback to AHAs.
The Framework (The workforce, 2012) states that “while AHAs are not autonomous practitioners and always work under the overarching auspice and clinical oversight of the AHP, the degree of monitoring required will vary depending on the knowledge, experience, skill level and Grade of the AHA”. On their website, Services for Australian Remote and Rural Allied Health (SARRAH) states that an “Allied Health Assistants (AHAs) must work under the supervision of the relevant Allied Health Professional (AHPs) (i.e. tasks must be delegated to them by an Allied Health Professional). The level of supervision and monitoring will depend on the experience, skill and qualifications of the assistant and the practicalities of the work environment. Supervision may range from face to face daily interaction to less frequently and by telephone or video”. In most cases the scope of practice for assistants stating what an AHA can and can’t do is guided by the employing organisational and professional associations/regulatory bodies.
According to the Framework (The Workforce, 2012. p.25) “supervision can vary in terms of what it covers” and “depending on the context,
complexity of the task or the needs of the patients” can incorporate any of the following elements:
1. Delegation- the act of giving control, responsibility, a task or a duty to another person, in this instance the AHP delegating a task/duty to an AHA
2. Direction- assistance in pointing out the proper course of action
3. Guidance- help or advice informing an AHA what to do : the act or process of guiding the AHA through visual, verbal, manual and/or
mechanical aids
4. Support- to reassure, nurture, protect, give help or assistance to the AHA enabling them to increase their skills and confidence
5. Observation- the act of careful watching and listening; the AHP pays close attention to the AHA in order to get information
6. Joint working – or joint problem-solving involving an ongoing relationship and two-way communication between AHP and AHA (such as in Supportive Supervision)
7. Exchanging ideas
8. Coordinating activities
To achieve implementation of an effective supervision model the following factors need to be kept in mind:
- “The environment in which learning takes place profoundly affects what is learnt and the learners' responses” (Kilminster& Jolly, 2000.
p.830).
- The availability of regular supervision sessions to support this interpersonal collaborative process which also includes uninterrupted sessions away from the clinical setting.
· - Accessibility of the supervisor for feedback and to ensures that the (clinical) supervision process is conducted in an expert manner in which ethical standards and professional practices and treatments are used to promote and protect the safety of the client and the allied health profession.
· - Supervision by the AHP should concentrate on all four areas of AHA competence:
# Knowledge and information – the AHA must understand how to effectively perform the duties of their job, which includes professional and ethical work standards as well as organisational policies and procedures.
# Work-related skills – AHAs need to remain current on developing trends within their field
of work and they should have the opportunity to develop and acquire new skills.
# Personal skills – which is part of an holistic approach to supervision.
# Attitudes- a positive attitude among AHAs assists with applying knowledge and/or skills to strive toward personal and department goals.
· # Ongoing AHP (supervisor) – AHA relationship.
- “The environment in which learning takes place profoundly affects what is learnt and the learners' responses” (Kilminster& Jolly, 2000.
p.830).
- The availability of regular supervision sessions to support this interpersonal collaborative process which also includes uninterrupted sessions away from the clinical setting.
· - Accessibility of the supervisor for feedback and to ensures that the (clinical) supervision process is conducted in an expert manner in which ethical standards and professional practices and treatments are used to promote and protect the safety of the client and the allied health profession.
· - Supervision by the AHP should concentrate on all four areas of AHA competence:
# Knowledge and information – the AHA must understand how to effectively perform the duties of their job, which includes professional and ethical work standards as well as organisational policies and procedures.
# Work-related skills – AHAs need to remain current on developing trends within their field
of work and they should have the opportunity to develop and acquire new skills.
# Personal skills – which is part of an holistic approach to supervision.
# Attitudes- a positive attitude among AHAs assists with applying knowledge and/or skills to strive toward personal and department goals.
· # Ongoing AHP (supervisor) – AHA relationship.
|
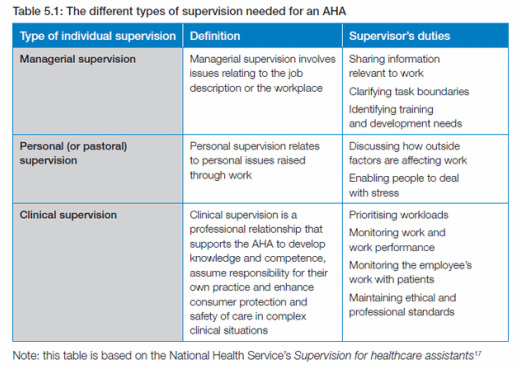
Types of Supervision The Framework describes three different types of supervision needed for an AHA: * managerial (normative) * personal (pastoral or restorative) * clinical supervision (educational or formative). |
|
Mode of Supervision
The mode of supervision is the way by which the AHP can supervise the AHA. According to the Framework (The Workforce, 2012. p.31) this can be in the form of :
The mode of supervision is the way by which the AHP can supervise the AHA. According to the Framework (The Workforce, 2012. p.31) this can be in the form of :
|
Direct supervision –
the supervisor works alongside the AHA and is able to observe and direct the activities of the AHA, enabling immediate guidance, feedback and intervention as required |
Indirect supervision –
the supervisor is not physically present, but processes are in place to ensure the supervisor is easily contactable and accessible to provide direction, guidance and support as required |
Remote supervision –
the supervisor is located some distance from the AHA, but processes are in place to ensure the supervisor is contactable and reasonably accessible to provide direction, guidance and support as required. |
Reasonable access and frequency of monitoring required as well as the supervision method used by the AHP are partly determined by the
skills and competence of the AHA.
skills and competence of the AHA.
References:
Kilminster, S.M. & Jolly, B.C. (2000). Effective supervision in clinical practice settings: a literature review. Medical Education 2000;34:827±840. Blackwell Science Ltd
Kleiser, H. & Cox, D.L. (2008). The Integration of Clinical and Managerial Supervision: a Critical Literature Review. British Journal of Occupational Therapy January 2008 71(1)
The Workforce (2012). Supervision and Delegation Framework for Allied Health Assistants. Department of Health (Victoria). Finsbury Green Printers
Winston & Creamer (2008). Supervision and managing staff. A Handbook for Staffing Practices in Student Affairs – University of Georgia. Retrieved April 2014 from: http://www.staffingpractices.soe.vt.edu/supervision.htm
Norway India Initiative Partnership. Supervision and monitoring: Health managers module for immunisation. National Institute of Health and Family Welfare, Delhi, India. Retrieved April 2014 from: http://www.nihfw.org/pdf/NCHRC-Publications/Module%20-%204.pdf
Marquez, L. & Kean, L. (2002). Making Supervision Supportive and Sustainable: New Approaches to Old Problems - Executive summary. USAID – MAQ Papers. Office of Population and Reproductive Health/Service Delivery Improvement Division USAID. Retrieved April 2014 from: https://www.k4health.org/sites/default/files/maqpaperonsupervision_0.pdf
Practice Supervision Workbook – Supervisor. Queensland Health Practice Supervision Program for Mental Health Practitioners. Retrieved April 2014 from: http://www.health.qld.gov.au/qcmhl/Supervision/SuperworkB.pdf
Providing quality feedback - a good practice guide. University of South Australia. People development and performance. Retrieved April 2014 from: http://w3.unisa.edu.au/staffdev/guides/good_practice_guide_to_providing_quality_feedback.pdf
Kilminster, S.M. & Jolly, B.C. (2000). Effective supervision in clinical practice settings: a literature review. Medical Education 2000;34:827±840. Blackwell Science Ltd
Kleiser, H. & Cox, D.L. (2008). The Integration of Clinical and Managerial Supervision: a Critical Literature Review. British Journal of Occupational Therapy January 2008 71(1)
The Workforce (2012). Supervision and Delegation Framework for Allied Health Assistants. Department of Health (Victoria). Finsbury Green Printers
Winston & Creamer (2008). Supervision and managing staff. A Handbook for Staffing Practices in Student Affairs – University of Georgia. Retrieved April 2014 from: http://www.staffingpractices.soe.vt.edu/supervision.htm
Norway India Initiative Partnership. Supervision and monitoring: Health managers module for immunisation. National Institute of Health and Family Welfare, Delhi, India. Retrieved April 2014 from: http://www.nihfw.org/pdf/NCHRC-Publications/Module%20-%204.pdf
Marquez, L. & Kean, L. (2002). Making Supervision Supportive and Sustainable: New Approaches to Old Problems - Executive summary. USAID – MAQ Papers. Office of Population and Reproductive Health/Service Delivery Improvement Division USAID. Retrieved April 2014 from: https://www.k4health.org/sites/default/files/maqpaperonsupervision_0.pdf
Practice Supervision Workbook – Supervisor. Queensland Health Practice Supervision Program for Mental Health Practitioners. Retrieved April 2014 from: http://www.health.qld.gov.au/qcmhl/Supervision/SuperworkB.pdf
Providing quality feedback - a good practice guide. University of South Australia. People development and performance. Retrieved April 2014 from: http://w3.unisa.edu.au/staffdev/guides/good_practice_guide_to_providing_quality_feedback.pdf
